



Spotlight
A selection of resources from across the Federation

Resource
IPPF Annual Report and Financial Statements 2025
Read our Annual Report and Financial Statements 2025.
Most Popular This Week

Resource
|
IPPF Annual Report and Financial Statements 2025
IPPF is a global federation and movement of 100+ locally led Member Associations and Collaborative Partnersin 150+ countries, dedicated to sexual and reproductive health, rights

Resource
|
Annual Performance Report 2025
The IPPF Annual Performance Report 2025 tells a story of resilience, solidarity and shared leadership across our Federation.


Resource
|
Review of IPPF’s Governance Reform
Following IPPF’s governance reform in 2019/2020, a review of the reform process was conducted, which provided important insights for the new Board of Trustees and the Secretariat to support the cha

Resource
|
IMAP Statement on Sex Worker-Centred Sexual and Reproductive Health Services
This statement is intended to provide guidance to Member Associations and Collaborative Partners across the Federation on delivering comprehensive, evidence‑based sexual and reproductive health (SR



Resource
|
IPPF in 2024: Financial Statements
We are a worldwide federation of national SRHR organizations working with and for communities and individuals. Our 119 Member Associations and 39 Collaborative Partners span 153 countries.
Filter our resources by:


Resource
| 28 July 2025
Feminist Principles in Humanitarian Contexts
This document outlines IPPF’s feminist approach to humanitarian action, rooted in rights-based, inclusive, and intersectional principles. It highlights the need to challenge structural inequalities, patriarchal norms, and colonial legacies in humanitarian systems while centring the voices of women, girls, LGBTQI+ communities, and other marginalised groups.The principles call for locally led, gender-transformative action, meaningful participation, and accountability to affected communities. With sexual and reproductive health and rights (SRHR) as a life-saving priority, IPPF advocates for integrated, community-driven humanitarian responses that uphold dignity, equity, and justice for all.
Resource
| 31 May 2024
Feminist Principles in Humanitarian Contexts
This document outlines IPPF’s feminist approach to humanitarian action, rooted in rights-based, inclusive, and intersectional principles. It highlights the need to challenge structural inequalities, patriarchal norms, and colonial legacies in humanitarian systems while centring the voices of women, girls, LGBTQI+ communities, and other marginalised groups.The principles call for locally led, gender-transformative action, meaningful participation, and accountability to affected communities. With sexual and reproductive health and rights (SRHR) as a life-saving priority, IPPF advocates for integrated, community-driven humanitarian responses that uphold dignity, equity, and justice for all.

Resource
| 22 July 2025
Annual Performance Report 2024
IPPF Annual Performance Report 2024IPPF Annual Performance Report 2024
Resource
| 22 July 2025
Annual Performance Report 2024
IPPF Annual Performance Report 2024IPPF Annual Performance Report 2024

Resource
| 21 July 2025
Abortion Education – Online Courses for Medical Abortion
Medical Abortion Course For ProvidersMedical abortion is a safe and common method of pregnancy termination. Healthcare workers can provide care during medical abortion either by directly overseeing the process or by supporting women to self-manage the abortion outside of a clinical setting. This course will review the necessary information and resources to ensure that women around the world have access to a safe and effective option for pregnancy termination. This course is created in collaboration with International Planned Parenthood Federation.Access the training here: Abortion Education - Online Course for Individuals
Resource
| 21 July 2025
Abortion Education – Online Courses for Medical Abortion
Medical Abortion Course For ProvidersMedical abortion is a safe and common method of pregnancy termination. Healthcare workers can provide care during medical abortion either by directly overseeing the process or by supporting women to self-manage the abortion outside of a clinical setting. This course will review the necessary information and resources to ensure that women around the world have access to a safe and effective option for pregnancy termination. This course is created in collaboration with International Planned Parenthood Federation.Access the training here: Abortion Education - Online Course for Individuals

Resource
| 18 July 2025
IPPF in 2024: Financial Statements
We are a worldwide federation of national SRHR organizations working with and for communities and individuals. Our 119 Member Associations and 39 Collaborative Partners span 153 countries. We are 73 years old and deeply rooted in our communities. Our work is wide-ranging. Among our many services, we offer comprehensive sexuality education, contraceptive provision, safe abortion and maternal care. We respond to SRHR needs in humanitarian and crisis settings, whether caused by climate change, political failures or natural phenomena. We cover most parts of the world, from community to global level. At the heart of our mission is the provision of – and advocacy in support of – integrated healthcare to anyone who needs it, but with a focus on those who are most marginalized.Download our 2024 Annual Report and Financial Statements below to learn about our work and impact worldwide.
Resource
| 18 July 2025
IPPF in 2024: Financial Statements
We are a worldwide federation of national SRHR organizations working with and for communities and individuals. Our 119 Member Associations and 39 Collaborative Partners span 153 countries. We are 73 years old and deeply rooted in our communities. Our work is wide-ranging. Among our many services, we offer comprehensive sexuality education, contraceptive provision, safe abortion and maternal care. We respond to SRHR needs in humanitarian and crisis settings, whether caused by climate change, political failures or natural phenomena. We cover most parts of the world, from community to global level. At the heart of our mission is the provision of – and advocacy in support of – integrated healthcare to anyone who needs it, but with a focus on those who are most marginalized.Download our 2024 Annual Report and Financial Statements below to learn about our work and impact worldwide.

Resource
| 02 June 2025
MA Connect
Introducing MA Connect – Your New Digital Space!We’re excited to launch MA Connect, the new name and improved platform for what was previously known as the IPPF Internal Social Media.MA Connect is a dedicated, password-protected website and mobile application designed exclusively for IPPF Member Associations and staff. It’s your space to share updates, exchange ideas, access resources, and connect with colleagues across the Federation – wherever you are in the world.With a fresh new name and enhanced features, MA Connect makes it easier than ever to:Stay informed about key Federation news and campaignsCollaborate and learn from peers across regionsShare your work and successesAccess useful tools and documentsJoin conversations on topics that matter to youAvailable on both desktop and mobile, MA Connect ensures you can engage with the IPPF community anytime, anywhere.Have a question or need support? Contact us at maforum@ippf.org.Let’s connect, collaborate, and grow – together.
Resource
| 02 June 2025
MA Connect
Introducing MA Connect – Your New Digital Space!We’re excited to launch MA Connect, the new name and improved platform for what was previously known as the IPPF Internal Social Media.MA Connect is a dedicated, password-protected website and mobile application designed exclusively for IPPF Member Associations and staff. It’s your space to share updates, exchange ideas, access resources, and connect with colleagues across the Federation – wherever you are in the world.With a fresh new name and enhanced features, MA Connect makes it easier than ever to:Stay informed about key Federation news and campaignsCollaborate and learn from peers across regionsShare your work and successesAccess useful tools and documentsJoin conversations on topics that matter to youAvailable on both desktop and mobile, MA Connect ensures you can engage with the IPPF community anytime, anywhere.Have a question or need support? Contact us at maforum@ippf.org.Let’s connect, collaborate, and grow – together.

Resource
| 30 May 2025
U.S. 990 2023
Download the IPPF's 2023 "Return of Organization Exempt From Income Tax" U.S. 990 report below
Resource
| 30 May 2025
U.S. 990 2023
Download the IPPF's 2023 "Return of Organization Exempt From Income Tax" U.S. 990 report below

Resource
| 12 May 2025
IMAP Statement on Advances in Emergency Contraception
The purpose of this statement is to review newly published data on increasing the effectiveness of levonorgestrel emergency contraceptive pills by using pre‑coital administration or combined with a non‑steroidal anti‑inflammatory drug; the potential use of LNG‑ECP as a regular contraceptive method for infrequent sex; ulipristal acetate which is an established EC method and is now being studied combined with misoprostol for termination of early pregnancy; and the underutilization of low dose mifepristone as an EC method.
Resource
| 12 May 2025
IMAP Statement on Advances in Emergency Contraception
The purpose of this statement is to review newly published data on increasing the effectiveness of levonorgestrel emergency contraceptive pills by using pre‑coital administration or combined with a non‑steroidal anti‑inflammatory drug; the potential use of LNG‑ECP as a regular contraceptive method for infrequent sex; ulipristal acetate which is an established EC method and is now being studied combined with misoprostol for termination of early pregnancy; and the underutilization of low dose mifepristone as an EC method.

Resource
| 21 March 2025
Technical Brief: Designing and Delivering Inclusive, Rights-Based Sexual and Reproductive Healthcare to Transgender and Gender Diverse People
IPPF’s commitment to person-centred care is at the heart of its strategy, Come Together (2023–2028). We deliver quality, rights-based care to all who need it, prioritizing services for marginalized communities. This entails offering options for care that are sensitive to people’s individual needs and lived experiences. It requires healthcare providers to be aware of clients’ needs and to respect their rights. This work advances IPPF’s vision of a world where all people are free to make choices about their sexuality and well-being, free from discrimination. Inclusive sexual and reproductive healthcare delivery to transgender and gender diverse people is founded upon the principles of the rights to personal autonomy, bodily integrity and respect for clients’ confidentiality and dignity. And yet, around the world, transgender and gender diverse people face widespread stigma, discrimination, violence and exclusion in healthcare settings. A crucial aspect of providing inclusive sexual and reproductive healthcare to transgender and gender diverse people therefore relates to strengthening the capacity and attitudes of healthcare providers and clinic staff as well as understanding the needs of transgender and gender diverse people. This technical brief outlines key recommendations across several sexual and reproductive health service areas to promote access to inclusive care for transgender and gender diverse people. Our goal is to expand the choice of existing or new quality sexual and reproductive health services for transgender and gender diverse people in facility and community settings.
Resource
| 21 March 2025
Technical Brief: Designing and Delivering Inclusive, Rights-Based Sexual and Reproductive Healthcare to Transgender and Gender Diverse People
IPPF’s commitment to person-centred care is at the heart of its strategy, Come Together (2023–2028). We deliver quality, rights-based care to all who need it, prioritizing services for marginalized communities. This entails offering options for care that are sensitive to people’s individual needs and lived experiences. It requires healthcare providers to be aware of clients’ needs and to respect their rights. This work advances IPPF’s vision of a world where all people are free to make choices about their sexuality and well-being, free from discrimination. Inclusive sexual and reproductive healthcare delivery to transgender and gender diverse people is founded upon the principles of the rights to personal autonomy, bodily integrity and respect for clients’ confidentiality and dignity. And yet, around the world, transgender and gender diverse people face widespread stigma, discrimination, violence and exclusion in healthcare settings. A crucial aspect of providing inclusive sexual and reproductive healthcare to transgender and gender diverse people therefore relates to strengthening the capacity and attitudes of healthcare providers and clinic staff as well as understanding the needs of transgender and gender diverse people. This technical brief outlines key recommendations across several sexual and reproductive health service areas to promote access to inclusive care for transgender and gender diverse people. Our goal is to expand the choice of existing or new quality sexual and reproductive health services for transgender and gender diverse people in facility and community settings.

Resource
| 10 March 2025
Sexual and gender-based violence services and programming overview brief
The International Planned Parenthood Federation (IPPF) is pleased to be share this Sexual and Gender-based Violence Services and Programming overview document. Globally, approximately one in three women are affected by sexual and gender-based violence (SGBV). At IPPF, we recognise that SGBV is a major public health issue, a clinical health problem, and a violation of human rights and is a key barrier to fully accessing sexual and reproductive healthcare. IPPF is dedicated to scaling up work at the community level, including in humanitarian contexts, to prevent and respond to SGBV. This document is intended to support and guide IPPF Member Associations (MAs) on how they can integrate their SGBV services and programmes throughout the four pillars of Strategy 2028 during stable times and during times of crisis.
Resource
| 10 March 2025
Sexual and gender-based violence services and programming overview brief
The International Planned Parenthood Federation (IPPF) is pleased to be share this Sexual and Gender-based Violence Services and Programming overview document. Globally, approximately one in three women are affected by sexual and gender-based violence (SGBV). At IPPF, we recognise that SGBV is a major public health issue, a clinical health problem, and a violation of human rights and is a key barrier to fully accessing sexual and reproductive healthcare. IPPF is dedicated to scaling up work at the community level, including in humanitarian contexts, to prevent and respond to SGBV. This document is intended to support and guide IPPF Member Associations (MAs) on how they can integrate their SGBV services and programmes throughout the four pillars of Strategy 2028 during stable times and during times of crisis.
Resource
| 07 February 2025
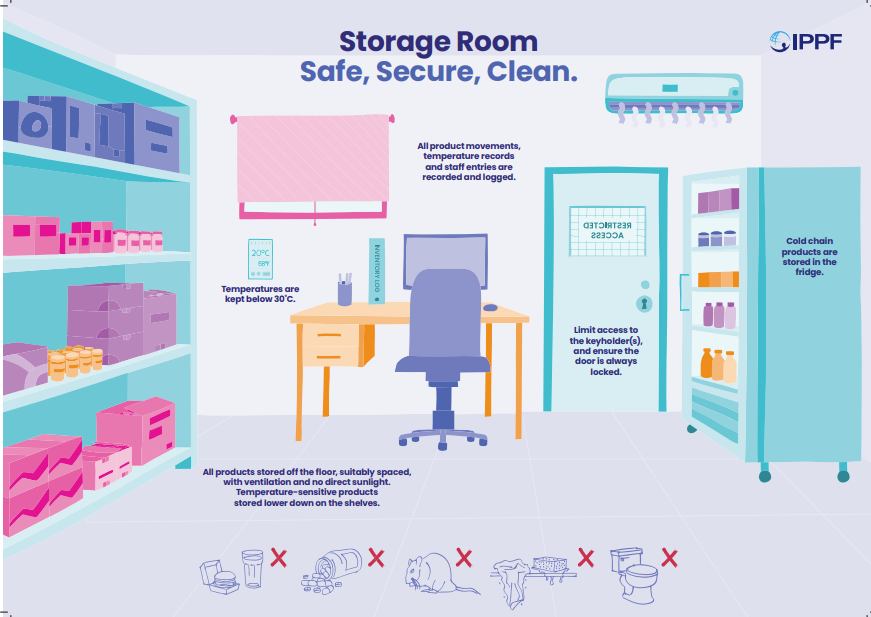
IPPF Storage Room poster
IPPF is pleased to be providing an important poster aimed at promoting safe and effective storage practices for medical supplies in your storage rooms. We understand that the quality, safety, and accessibility of medical products depend heavily on proper storage protocols. The poster covers critical areas and provides straightforward recommendations to maintain storage room conditions that prioritize patient safety and the integrity of medicines, including temperature control, cleanliness, safety and security and efficient processes. By following these practices, we can collectively safeguard product quality, enhance efficiency, and contribute to better health outcomes. The poster is double-sided with an illustrative and informative side. We are therefore sharing with you the equivalent of two posters for each of your service delivery points. We encourage you to place both side of the poster in a visible location within your facilities as a reminder of these crucial storage standards.
Resource
| 07 February 2025
IPPF Storage Room poster
IPPF is pleased to be providing an important poster aimed at promoting safe and effective storage practices for medical supplies in your storage rooms. We understand that the quality, safety, and accessibility of medical products depend heavily on proper storage protocols. The poster covers critical areas and provides straightforward recommendations to maintain storage room conditions that prioritize patient safety and the integrity of medicines, including temperature control, cleanliness, safety and security and efficient processes. By following these practices, we can collectively safeguard product quality, enhance efficiency, and contribute to better health outcomes. The poster is double-sided with an illustrative and informative side. We are therefore sharing with you the equivalent of two posters for each of your service delivery points. We encourage you to place both side of the poster in a visible location within your facilities as a reminder of these crucial storage standards.
Resource
| 28 July 2025
Feminist Principles in Humanitarian Contexts
This document outlines IPPF’s feminist approach to humanitarian action, rooted in rights-based, inclusive, and intersectional principles. It highlights the need to challenge structural inequalities, patriarchal norms, and colonial legacies in humanitarian systems while centring the voices of women, girls, LGBTQI+ communities, and other marginalised groups.The principles call for locally led, gender-transformative action, meaningful participation, and accountability to affected communities. With sexual and reproductive health and rights (SRHR) as a life-saving priority, IPPF advocates for integrated, community-driven humanitarian responses that uphold dignity, equity, and justice for all.
Resource
| 31 May 2024
Feminist Principles in Humanitarian Contexts
This document outlines IPPF’s feminist approach to humanitarian action, rooted in rights-based, inclusive, and intersectional principles. It highlights the need to challenge structural inequalities, patriarchal norms, and colonial legacies in humanitarian systems while centring the voices of women, girls, LGBTQI+ communities, and other marginalised groups.The principles call for locally led, gender-transformative action, meaningful participation, and accountability to affected communities. With sexual and reproductive health and rights (SRHR) as a life-saving priority, IPPF advocates for integrated, community-driven humanitarian responses that uphold dignity, equity, and justice for all.
Resource
| 22 July 2025
Annual Performance Report 2024
IPPF Annual Performance Report 2024IPPF Annual Performance Report 2024
Resource
| 22 July 2025
Annual Performance Report 2024
IPPF Annual Performance Report 2024IPPF Annual Performance Report 2024
Resource
| 21 July 2025
Abortion Education – Online Courses for Medical Abortion
Medical Abortion Course For ProvidersMedical abortion is a safe and common method of pregnancy termination. Healthcare workers can provide care during medical abortion either by directly overseeing the process or by supporting women to self-manage the abortion outside of a clinical setting. This course will review the necessary information and resources to ensure that women around the world have access to a safe and effective option for pregnancy termination. This course is created in collaboration with International Planned Parenthood Federation.Access the training here: Abortion Education - Online Course for Individuals
Resource
| 21 July 2025
Abortion Education – Online Courses for Medical Abortion
Medical Abortion Course For ProvidersMedical abortion is a safe and common method of pregnancy termination. Healthcare workers can provide care during medical abortion either by directly overseeing the process or by supporting women to self-manage the abortion outside of a clinical setting. This course will review the necessary information and resources to ensure that women around the world have access to a safe and effective option for pregnancy termination. This course is created in collaboration with International Planned Parenthood Federation.Access the training here: Abortion Education - Online Course for Individuals
Resource
| 18 July 2025
IPPF in 2024: Financial Statements
We are a worldwide federation of national SRHR organizations working with and for communities and individuals. Our 119 Member Associations and 39 Collaborative Partners span 153 countries. We are 73 years old and deeply rooted in our communities. Our work is wide-ranging. Among our many services, we offer comprehensive sexuality education, contraceptive provision, safe abortion and maternal care. We respond to SRHR needs in humanitarian and crisis settings, whether caused by climate change, political failures or natural phenomena. We cover most parts of the world, from community to global level. At the heart of our mission is the provision of – and advocacy in support of – integrated healthcare to anyone who needs it, but with a focus on those who are most marginalized.Download our 2024 Annual Report and Financial Statements below to learn about our work and impact worldwide.
Resource
| 18 July 2025
IPPF in 2024: Financial Statements
We are a worldwide federation of national SRHR organizations working with and for communities and individuals. Our 119 Member Associations and 39 Collaborative Partners span 153 countries. We are 73 years old and deeply rooted in our communities. Our work is wide-ranging. Among our many services, we offer comprehensive sexuality education, contraceptive provision, safe abortion and maternal care. We respond to SRHR needs in humanitarian and crisis settings, whether caused by climate change, political failures or natural phenomena. We cover most parts of the world, from community to global level. At the heart of our mission is the provision of – and advocacy in support of – integrated healthcare to anyone who needs it, but with a focus on those who are most marginalized.Download our 2024 Annual Report and Financial Statements below to learn about our work and impact worldwide.
Resource
| 02 June 2025
MA Connect
Introducing MA Connect – Your New Digital Space!We’re excited to launch MA Connect, the new name and improved platform for what was previously known as the IPPF Internal Social Media.MA Connect is a dedicated, password-protected website and mobile application designed exclusively for IPPF Member Associations and staff. It’s your space to share updates, exchange ideas, access resources, and connect with colleagues across the Federation – wherever you are in the world.With a fresh new name and enhanced features, MA Connect makes it easier than ever to:Stay informed about key Federation news and campaignsCollaborate and learn from peers across regionsShare your work and successesAccess useful tools and documentsJoin conversations on topics that matter to youAvailable on both desktop and mobile, MA Connect ensures you can engage with the IPPF community anytime, anywhere.Have a question or need support? Contact us at maforum@ippf.org.Let’s connect, collaborate, and grow – together.
Resource
| 02 June 2025
MA Connect
Introducing MA Connect – Your New Digital Space!We’re excited to launch MA Connect, the new name and improved platform for what was previously known as the IPPF Internal Social Media.MA Connect is a dedicated, password-protected website and mobile application designed exclusively for IPPF Member Associations and staff. It’s your space to share updates, exchange ideas, access resources, and connect with colleagues across the Federation – wherever you are in the world.With a fresh new name and enhanced features, MA Connect makes it easier than ever to:Stay informed about key Federation news and campaignsCollaborate and learn from peers across regionsShare your work and successesAccess useful tools and documentsJoin conversations on topics that matter to youAvailable on both desktop and mobile, MA Connect ensures you can engage with the IPPF community anytime, anywhere.Have a question or need support? Contact us at maforum@ippf.org.Let’s connect, collaborate, and grow – together.
Resource
| 30 May 2025
U.S. 990 2023
Download the IPPF's 2023 "Return of Organization Exempt From Income Tax" U.S. 990 report below
Resource
| 30 May 2025
U.S. 990 2023
Download the IPPF's 2023 "Return of Organization Exempt From Income Tax" U.S. 990 report below
Resource
| 12 May 2025
IMAP Statement on Advances in Emergency Contraception
The purpose of this statement is to review newly published data on increasing the effectiveness of levonorgestrel emergency contraceptive pills by using pre‑coital administration or combined with a non‑steroidal anti‑inflammatory drug; the potential use of LNG‑ECP as a regular contraceptive method for infrequent sex; ulipristal acetate which is an established EC method and is now being studied combined with misoprostol for termination of early pregnancy; and the underutilization of low dose mifepristone as an EC method.
Resource
| 12 May 2025
IMAP Statement on Advances in Emergency Contraception
The purpose of this statement is to review newly published data on increasing the effectiveness of levonorgestrel emergency contraceptive pills by using pre‑coital administration or combined with a non‑steroidal anti‑inflammatory drug; the potential use of LNG‑ECP as a regular contraceptive method for infrequent sex; ulipristal acetate which is an established EC method and is now being studied combined with misoprostol for termination of early pregnancy; and the underutilization of low dose mifepristone as an EC method.
Resource
| 21 March 2025
Technical Brief: Designing and Delivering Inclusive, Rights-Based Sexual and Reproductive Healthcare to Transgender and Gender Diverse People
IPPF’s commitment to person-centred care is at the heart of its strategy, Come Together (2023–2028). We deliver quality, rights-based care to all who need it, prioritizing services for marginalized communities. This entails offering options for care that are sensitive to people’s individual needs and lived experiences. It requires healthcare providers to be aware of clients’ needs and to respect their rights. This work advances IPPF’s vision of a world where all people are free to make choices about their sexuality and well-being, free from discrimination. Inclusive sexual and reproductive healthcare delivery to transgender and gender diverse people is founded upon the principles of the rights to personal autonomy, bodily integrity and respect for clients’ confidentiality and dignity. And yet, around the world, transgender and gender diverse people face widespread stigma, discrimination, violence and exclusion in healthcare settings. A crucial aspect of providing inclusive sexual and reproductive healthcare to transgender and gender diverse people therefore relates to strengthening the capacity and attitudes of healthcare providers and clinic staff as well as understanding the needs of transgender and gender diverse people. This technical brief outlines key recommendations across several sexual and reproductive health service areas to promote access to inclusive care for transgender and gender diverse people. Our goal is to expand the choice of existing or new quality sexual and reproductive health services for transgender and gender diverse people in facility and community settings.
Resource
| 21 March 2025
Technical Brief: Designing and Delivering Inclusive, Rights-Based Sexual and Reproductive Healthcare to Transgender and Gender Diverse People
IPPF’s commitment to person-centred care is at the heart of its strategy, Come Together (2023–2028). We deliver quality, rights-based care to all who need it, prioritizing services for marginalized communities. This entails offering options for care that are sensitive to people’s individual needs and lived experiences. It requires healthcare providers to be aware of clients’ needs and to respect their rights. This work advances IPPF’s vision of a world where all people are free to make choices about their sexuality and well-being, free from discrimination. Inclusive sexual and reproductive healthcare delivery to transgender and gender diverse people is founded upon the principles of the rights to personal autonomy, bodily integrity and respect for clients’ confidentiality and dignity. And yet, around the world, transgender and gender diverse people face widespread stigma, discrimination, violence and exclusion in healthcare settings. A crucial aspect of providing inclusive sexual and reproductive healthcare to transgender and gender diverse people therefore relates to strengthening the capacity and attitudes of healthcare providers and clinic staff as well as understanding the needs of transgender and gender diverse people. This technical brief outlines key recommendations across several sexual and reproductive health service areas to promote access to inclusive care for transgender and gender diverse people. Our goal is to expand the choice of existing or new quality sexual and reproductive health services for transgender and gender diverse people in facility and community settings.
Resource
| 10 March 2025
Sexual and gender-based violence services and programming overview brief
The International Planned Parenthood Federation (IPPF) is pleased to be share this Sexual and Gender-based Violence Services and Programming overview document. Globally, approximately one in three women are affected by sexual and gender-based violence (SGBV). At IPPF, we recognise that SGBV is a major public health issue, a clinical health problem, and a violation of human rights and is a key barrier to fully accessing sexual and reproductive healthcare. IPPF is dedicated to scaling up work at the community level, including in humanitarian contexts, to prevent and respond to SGBV. This document is intended to support and guide IPPF Member Associations (MAs) on how they can integrate their SGBV services and programmes throughout the four pillars of Strategy 2028 during stable times and during times of crisis.
Resource
| 10 March 2025
Sexual and gender-based violence services and programming overview brief
The International Planned Parenthood Federation (IPPF) is pleased to be share this Sexual and Gender-based Violence Services and Programming overview document. Globally, approximately one in three women are affected by sexual and gender-based violence (SGBV). At IPPF, we recognise that SGBV is a major public health issue, a clinical health problem, and a violation of human rights and is a key barrier to fully accessing sexual and reproductive healthcare. IPPF is dedicated to scaling up work at the community level, including in humanitarian contexts, to prevent and respond to SGBV. This document is intended to support and guide IPPF Member Associations (MAs) on how they can integrate their SGBV services and programmes throughout the four pillars of Strategy 2028 during stable times and during times of crisis.
Resource
| 07 February 2025
IPPF Storage Room poster
IPPF is pleased to be providing an important poster aimed at promoting safe and effective storage practices for medical supplies in your storage rooms. We understand that the quality, safety, and accessibility of medical products depend heavily on proper storage protocols. The poster covers critical areas and provides straightforward recommendations to maintain storage room conditions that prioritize patient safety and the integrity of medicines, including temperature control, cleanliness, safety and security and efficient processes. By following these practices, we can collectively safeguard product quality, enhance efficiency, and contribute to better health outcomes. The poster is double-sided with an illustrative and informative side. We are therefore sharing with you the equivalent of two posters for each of your service delivery points. We encourage you to place both side of the poster in a visible location within your facilities as a reminder of these crucial storage standards.
Resource
| 07 February 2025
IPPF Storage Room poster
IPPF is pleased to be providing an important poster aimed at promoting safe and effective storage practices for medical supplies in your storage rooms. We understand that the quality, safety, and accessibility of medical products depend heavily on proper storage protocols. The poster covers critical areas and provides straightforward recommendations to maintain storage room conditions that prioritize patient safety and the integrity of medicines, including temperature control, cleanliness, safety and security and efficient processes. By following these practices, we can collectively safeguard product quality, enhance efficiency, and contribute to better health outcomes. The poster is double-sided with an illustrative and informative side. We are therefore sharing with you the equivalent of two posters for each of your service delivery points. We encourage you to place both side of the poster in a visible location within your facilities as a reminder of these crucial storage standards.
